| Key
Facts |
- Autoimmune disorder
- Commonly associated
with other connective tissue diseases (secondary SS)
- Affects middle
aged females
- Widespread tissue
infiltration by polyclonal B-lymphocytes
- Keratoconjunctivitis
sicca, xerostomia, recurrent swelling of the parotid gland
- Radiography: interstitial
lung disease (UIP, LIP), cystic lung disease, recurrent pneumonias,
airway disease
- Increased risk
for pseudolymphoma and lymphoma
|
| Imaging
Findings |
Chest
radiography
- CXR abnormal (<
33%)
- Reticulonodular
pattern, basal predominance (most common)
- Bronchial wall
thickening, bronchiectasis
- Recurrent bronchopneumonias
- Atelectasis
- Pleural effusion
or thickening (uncommon)
- Pulmonary artery
hypertension (uncommon)
- Lymphadenopathy
suggests pseudolymphoma or malignant lymphoma
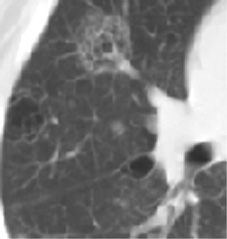
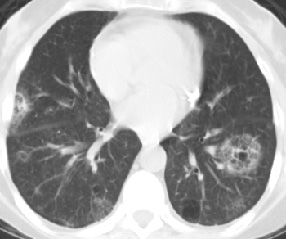
CT/HRCT
- Basal predominance
- Bronchiolectasis,
centrilobular nodules or branching opacities
- Mosaic attenuation,
air trapping
- Thin-walled cysts
(5 – 30 mm)
- Linear opacities
(septal and nonseptal)
- Airspace opacities
– bronchopneumonia or pseudolymphoma
- Pleural effusion
or thickening (uncommon)
|
| Differential
Diagnosis |
- UIP
- Collagen vascular
disease
- Drug reaction
- Asbestosis
- Cystic disease
- Langerhans cell
granulomatosis
- Tuberous sclerosis
- Lymphangiomyomatosis
- Pneumocystis
carinii pneumonia
|
| Pathological
Features |
- Autoimmune process
- Possible viral
etiology: EB, hepatitic C, herpes, retrovirus
- Infiltration of
tissues with polyclonal B-lymphocytes
- Lymphocytic infiltration,
glandular atrophy, impaired secretion of lacrimal, salivary, airway
mucous glands
- Pleuropulmonary
abnormalities (30%):
- Airway disease
- Tracheobronchitis
- Follicular
bronchiolitis (peribronchiolar lymphoplasmacytic infiltrates)
- BOOP
- Recurrent pneumonias
- Interstitial
lung disease (33%)
- LIP (diffuse)
- Pseudolymphoma
(localized)
- UIP
- Pleuritis with
or without effusion, pleural thickening (10%)
- Lymphadenitis
- Plexogenic pulmonary
arteriopathy (rare)
- Amyloidosis
- Systemic necrotizing
vasculitis, small and large vessels
- Risk for non-Hodgkins
lymphoma
|
| Clinical
Presentation |
- Females (90%),
mean age 57 years
- Sicca syndrome:
dry eyes, mouth, nose
- Lacrimal, submandibular
and parotid gland enlargement
- Hoarseness, cough,
pleuritic pain, dyspnea
- Recurrent infections,
bronchitis, pneumonia (secondary to impaired secretions)
- Associated with
other autoimmune diseases: chronic active hepatitis, primary biliary
cirrhosis, Hashimoto’s thyroiditis, myasthenia gravis, celiac
disease, renal tubular disorders, myopathy, neuropathy, CNS disorders,
Raynaud’s, vasculitis,purpura,
polyarthropathy, thrombocytopenic purpura (rare) hypothyroidism, splenomegaly
- (50-67%) have connective
tissue disease (secondary SS)
- Secondary SS associated
with RA, PSS, SLE, polymyositis
- Positive RF (90%),
ANA (70%)
- Lymphopenia, leukopenia,
polyclonal gammopathy IgG, IgM
- Diagnosis
- Sicca syndrome
- Abnormal Schirmer’s
test/Rose Bengal test
- Biopsy of minor
salivary glands
- Parotid sialography
- Detection of
antibodies to extractable nuclear antigens (SS-A, SS-B)
- PFTs - obstructuve,
restrictive, or diffusion abnormalities; hyperresponsive airway
- BAL – lymphocytosis
- Both primary and
secondary SS – increased risk for pseudolymphoma, lymphoma
- Prognosis, poorly
described
- Primary SS,
may progress rapidly
|
| References |
Strimlan
CV, Rosenow EC, 3rd, Divertie MB, et al. Pulmonary manifestations of Sjogren's
syndrome Chest 70:354-361, 1976
Meyer CA, Pina JS, Taillon D, et al. Inspiratory and expiratory high-resolution
CT findings in a patient with Sjogren's syndrome and cystic lung disease
AJR 168:101-103, 1997
|