| Key
Facts |
- Edema pattern,
acutely develop central-basilar consolidation
- Evolves to interstitial
thickening over 3 days and clears over 12 days
- Etiology: Both
immune and nonimmune
- Common causes:
Goodpasture’s, Idiopathic pulmonary hemosiderosis, vasculitis,
bone marrow transplantation (BMT)
- Iron deficiency
anemia
- Hemoptysis in 80%
(importantly may be absent)
|
| Imaging
Findings |
Chest
radiograph
- Acute basilar
consolidation, resembles pulmonary edema
- Evolution
- Slower to clear
than pulmonary edema, evolves over 3 days into reticular interstitial
thickening
- Interstitial
thickening in turn resolves over 12 days
- With repeated
hemorrhage, interstitial thickening becomes permanent
- May have small
effusions
- Adenopathy may
be seen in idiopathic pulmonary hemosiderosis
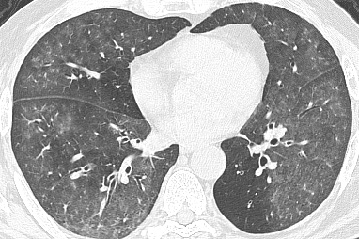
CT/HRCT
- Spectrum of opacities
from focal ground glass to diffuse consolidation
- Subacute: 1-3mm
micronodules and interlobular septal thickening
MRI
- Hemorrhage –
intermediate signal TA
- Low signal T2
(iron susceptibility effect)
|
| Differential
Diagnosis |
- Cardiogenic pulmonary
edema
- Infection
- BOOP
- Chronic interstitial
lung disease (IPF, asbestosis, collagen vascular disease, drug reaction)
|
| Pathological
Features |
- Alveolar spaces
filled with blood
- Hemosiderin-laden
macrophages, key finding in BAL
- Septal fibrosis
with chronic hemorrhage
|
| Clinical
Presentation |
- Nonspecific cough,
dyspnea
- Hemoptysis in 80%
- Iron deficiency
anemia
|
| References |
Albeida
SM et al. Diffuse pulmonary hemorrhage: a review and classification. Radiology
154: 289-97, 1985 |