| Key
Facts |
- Synonym: proliferative
bronchiolitis obliterans
- Patchy peripheral
consolidation, slight preference for lower lung zones
- Other patterns:
lobular sized nodules, solitary mass, diffuse interstitial thickening
- Causes: idiopathic,
infection, drugs, transplants, toxic fume inhalation
- Cough, SOB, low
grade fever
- Restrictive pulmonary
function tests
- Steroid responsive
|
| Imaging
Findings |
| Chest
radiograph
- Patchy, bilateral
variable sized areas of consolidation
- Unilateral 5%
- Favors the lower
lung zones
- Normal heart size,
no adenopathy
- Lung volumes preserved
- Less common: solitary
mass (usually upper lung zone)
- Less common: diffuse
reticular interstital thickening
- May wax and wane
(also termed migration)
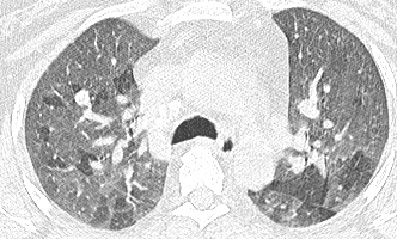
CT/HRCT
- Peripheral opacities
range from ground glass density to consolidation
- Consolidation often
triangular in shape
- Consolidation may
extend along bronchi (peribronchovascular pattern)
- Mild mediastinal
adenopathy common (not seen chest radiographs)
- Lobular sized nodules
with well defined margins in random distribution
- Diffuse reticular
interstitial thickening primarily basilar, less common
- Solitary mass may
have air bronchograms or cavitate, usually upper lobe location
- Occasional small
effusion
|
| Differential
Diagnosis |
- Chronic eosinophilic
pneumonia
- Usual interstital
pneumonia (UIP)
- Lymphoma
- Bronchioloalveolar
cell carcinoma (BAC)
- Sarcoid
- Lung cancer (solitary
mass)
- Mycobacterial infection
- Lipoid pneumonia
- Differentiation
- Eosinophilic
pneumonia usually upper lung zone, eosinophilia absent in BOOP
- UIP- honeycombing
and decreased lung volumes absent in BOOP
- Solitary form
usually resected on premise that it is lung cancer
- Lymphoma and
BAC not peripherally predominant, BAC usually ground glass density
- Lipoid pneumonia
may have fat density in areas of consolidated lung at CT
|
| Pathological
Features |
- Buds of loosely organized
granulation tissue extends through pores of Kohn to next alveolus (“butterfly”
pattern)
- Granulation tissue extends
into airway lumen (Bronchiolitis component)
- Mononuclear cell interstitial
infiltration
- Lung architecture preserved
(no fibrosis)
Causes
- Idiopathic
- Infection (mycoplasma,
viruses, atypical bacteria)
- Drugs (amiodarone, bleomycin,
sulfasalazine)
- Connective tissue disease
(rheumatoid arthritis, Sjögrens)
- Transplant (lung, bone
marrow)
- Toxic fume inhalation
(silo fillers disease)
- Radiation therapy
- Aspiration
- Wegener’s
|
| Clinical
Presentation |
- Adults, no gender preference
- Cough
- SOB
- Low grade fever
- PFT’s usually restrictive,
maybe mixed restrictive and obstructive
Treatment
- Steroids, less dramatic
response then eosinophilic pneumonia
- Resolves over period
of weeks
- May relapse
on discontinuation of steroids
|
| References |
Davison
AG, Heard BE, McAllister WA, et al. Cryptogenic organizing pneumonitis
Q J Med 52:382-394, 1983
Lee KS, Kullnig P, Hartman TE, et al. Cryptogenic organizing pneumonia:
CT findings in 43 patients AJR 162:543-546, 1994
Cordier JF. Organising pneumonia Thorax 55:318-328, 2000
|