| Key
Facts |
- Chest usually
normal in acute, subacute disease
- Midlung fibrosis
in chronic disease
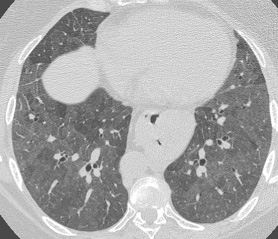
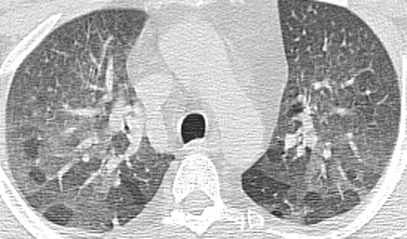
- HRCT: centrilobular
ground glass nodules with air trapping
- Usually spares
costophrenic angles
- Allergic reaction
organic antigens especially thermophilic actinomycetes
- Nonspecific flu
like symptoms
- Often misdiagnosed
as “pneumonia’
|
| Imaging
Findings |
Chest
Radiograph
- Often normal especially
acute and subacute forms
- Miliary disease
- Chronic: midlung
to upper lung zone fibrosis, bronchiectasis, and volume loss
- No pleural disease
or adenopathy
CT/HRCT
- More sensitive
but may be normal
- Ground glass centrilobular
nodules acutely
- Most prominent
med to lower lungs
- Air trapping common
- Spares costophrenic
angles
|
| Differential
Diagnosis |
- Idiopathic pulmonary
fibrosis
- Eosinophilic granuloma
- Sarcoid
- Pneumoconiosis
- Scleroderma
- Differentiation
- IPF does not
spare costophrenic angles
- EG nodules may
cavitate
- Patients with
EG smoke, smoking less common in hypersensitivity pneumonitis
- Sarcoid peribronchovascular
distribution
- Pneumoconiosis:
dust history, may have adenopathy
- Scleroderma,
dilated esophagus
|
| Pathological
Features |
- Airborne organic
particles (1-5 um)
- Thermophilic actinomycetes
- Exposure
- Farmer’s
lung
- Pigeon breeders
lung
- Humidifier
lung
- Loosley formed
noncaseating granulomas
- Lymphocytic infiltration
- BOOP
|
| Clinical
Presentation |
- Acute, subacute,
chronic forms, considerable overlap
- Nonspecific symptoms
- Often mistaken
as pneumonia
- Patient removed
from environment
- Gets well with
antibiotic treatment
- Cough, dyspnea,
fever 4-6 hours following exposure
- Individual must
be susceptible (allergic response), most dust exposed individuals have
no response
- Treatment
- Removal from
environment
- Steroids
|
| References |
Lynch
DA, Newell JD, Logan PM, et al. Can CT distinguish hypersensitivity pneumonitis
from idiopathic pulmonary fibrosis? AJR 165:807-811, 1995
Matar LD, McAdams HP , Sporn TA. Hypersensitivity pneumonitis AJR 174:1061-1066,
2000
|