| Key
Facts |
- Common disease,
any hospitalized patient at risk
- Chest radiograph
nonspecific, 10% normal
- Pulmonary infarcts
may be any shape or size
|
| Imaging
Findings |
Chest
radiograph
- 10% normal
- Most abnormalities
nonspecific
- Vascular enlargement
central pulmonary artery (knuckle sign)
- Focal oligemia
(Westermark sign)
- Pulmonary infarct
- 10% embolic
episodes result in infarction
- Infarction
more common in those with underlying cardiopulmonary disease
- May develop
immediately or delayed 2-3 days following embolus
- Any size or
shape but classically cone shaped in periphery of lower lobes
- Often associated
with small pleural effusion
- Evolution:
initially ill-defined, over time become sharply defined
- 50% clear completely
usually within 3 weeks
- May leave linear
scars (Fleischner lines)
CT/HRCT
- Directly visualize
clot in central pulmonary artery
- CT angiograms highly
sensitive and specific
- High observer agreement
- Outcomes of negative
CT angiograms excellent
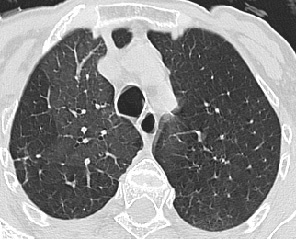
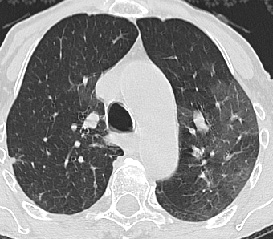
- Mosaic perfusion,
usually less well defined than pattern with small airways disease
- Due to vascular
obstruction with areas of hypoperfusion and overperfusion
- No air trapping
with expiratory scanning
|
| Differential
Diagnosis |
- Mosaic pattern
- Small airways
disease
- Viral or PCP
pneumonia
- Pulmonary alveolar
proteinosis
|
| Pathological
Features |
- Pulmonary emboli
end result of thrombosis in peripheral veins generally in the legs or
pelvis
|
| Clinical
Presentation |
- No telltale signs,
symptoms, or laboratory studies that strongly suggest PE
- Treatment
- Anticoagulation
and fibrinolysis
- IVC filters
if contraindications to drug therapy
- Prognosis
- Good with appropriate
therapy
- Mortality of
untreated disease 20%
|
| References |
Remy-Jardin
M et al: Spiral CT angiography of the pulmonary circulation. Radiology
212: 615-36, 1999
|