| Key
Facts |
- Aspiration of
oily substances, such as mineral oil, oil based nose drops or Vicks
VapoRub
- History of lipid
use may be difficult to illicit from patient
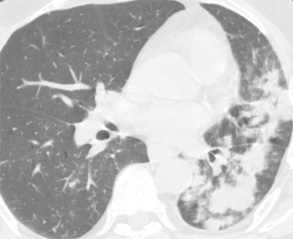
- Radiographically,
may be incidental finding of single or multiple irregular areas of consolidation
in dependent lung
- Diagnosis can be
made with CT if can demonstrate fatty tissue attenuation.
- Lipid laden macrophages
may be seen in BAL fluid
- Patient usually
asymtomatic but may have chronic cough
- Transthoracic needle
biopsy can provide definitive diagnosis
|
| Imaging
Findings |
General
Imaging findings
Early
- Airspace opacification,
confluent or discrete with air bronchograms
- May be large areas
with stellate or well-defined margins
- In dependent lung,
often segmental and in lower lobes
- In debilitated
patients – in posterior segments of upper lobes and superior segments
of lower lobes
Chronic
- Multifocal basal
mass-like areas of consolidation with irregular margins
- Cicatricial volume
loss in affected areas
- Interstitial pattern
- Well-circumscribed
peripheral mass
- Gravity dependent
lung segments
CT/HRCT
- Diagnosis made
with CT when the opacities show fatty attenuation, –50 to –150
HU
- Lesions may have
some ossification
- Lipoid etiology
not apparent when interstitial pattern predominates
- Mixed ground glass
and interlobular septal thickening may simulate alveolar proteinosis
- Fat may shift to
dependent lung with postural change
MR findings
- MR may show fat
- high T1 and T2 signal or chemical shift
|
| Differential
Diagnosis |
- Hamartoma
- Inflammatory pseudotumor
- Bronchiolitis obliterans
organizing pneumonia (BOOP)
- Bronchogenic carcinoma
- Alveolar proteinosis
- Differentiation
- Hamartoma may
have fatty attenuation with CT. Usually solitary mass, < 4 cm and
may have popcorn calcification
- Inflammatory
pseudotumor, BOOP, bronchogenic carcinoma and alveolar proteinosis
show no fatty attenuation at CT
|
| Pathological
Features |
- Mineral oil is
most common agent, but may occur with animal or vegetable oils.
- Initial reaction
is a bronchopneumonia. Macrophages ingest the lipid
- Clearing occurs
by mucociliary transport or macrophage migration via the interstitium
and lymphatics to mediastinal lymph nodes.
- Giant cell or granuloma
formation may occur.
- With mineral oil
aspiration, there are oil droplets within multinucleated giant cells,
lymphocytes and fibrous tissue
- Chronically, lipid
is fibrogenic
|
| Clinical
Presentation |
- Aspiration of oil
used as a lubricant in infants with feeding problems
- Aspiration of mineral
oil used for constipation in elderly
- Neurological or
esophageal disease may promote aspiration
- Oil not irritant,
aspiration often “silent”
- Most patients are
asymptomatic and do not offer history of lipid use
- Commonly discovered
as an incidental radiographic abnormality
- May have acute
pneumonia with large amount of aspirated material
- Chronic cough
- Diagnosis by recovering
lipid laden macrophages in BAL fluid or transthoracic needle biopsy
- Radiographic findings
may disappear with discontinuation of use of lipoid agent
- Small amount aspirated
– little impairment
- Large amounts –
may develop restrictive lung disease or cor pulmonale
- May increase risk
for bronchogenic carcinoma and nontuberculous mycobacterial infection
|
| References |
Seo
JB, Im JG, Kim WS, et al. Shark liver oil-induced lipoid pneumonia in
pigs: correlation of thin-section CT and histopathologic findings Radiology
212:88-96, 1999
Van den Plas O, Trigaux JP, Van Beers B, et al. Gravity-dependent infiltrates
in a patient with lipoid pneumonia Chest 98:1253-1254, 1990
Wheeler PS, Stitik FP, Hutchins GM, et al. Diagnosis of lipoid pneumonia
by computed tomography Jama 245:65-66, 1981
|
.jpg)