| Key
Facts |
- Miners inhaling
quartz (silica) or coal dust
- Radiography of
silicosis and CWP are similar:
- Simple: micronodules
< 1 cm, upper lungs, hilar/mediastinal lymphadenopathy, egg shell
calcifications
- Complicated
known as progessive massive fibrosis (PMF): aggregation of nodules
into large masses, may cavitate
- As PMF worsens
profusion of nodules decreases
- Acute silicoproteinosis:
resembles alveolar proteinosis, progresses to fibrosis
- Caplans syndrome:
CWP + rheumatoid arthritis + necrobiotic nodules
- Silicosis: round
lamellated collagen surrounding silica particles
- CWP: coal macule
composed of black pigmented macrophages in respiratory brnochioles
- Increased risk
for TB
- Requires 20 or
more years of high dust exposure, silicosis will progress, even after
removal from dust in contrast to CWP
- Increased mortality
with PMF
|
| Imaging
Findings |
Chest
radiography
- Findings seen 10
to 20 years after exposure
- Silicosis and CWP
similar, usually less severe in CWP
- Simple silicosis
- 1 – 3
mm nodules, posterior segments, upper lobes
- Nodules may
calcify
- Reticular opacities
- Nodules increase
in size and number and may eventually involve all lobes
- Hilar and mediastinal
lymphadenopathy, egg shell calcification
- Complicated silicosis
(PMF)
- Nodules coalesce
and are > 1 cm
- Usually bilateral,
right > left
- Usually located
in dorsal aspect of lung
- PMF may be
lens shaped (wide PA and narrow lateral view)
- Overall profusion
of nodules decreases due to aggregation into PMF
- May have foci
of amorphous calcification, or calcified rim
- Migrates centrally
with time
- May cavitate
- Lung distal
to PMF emphysematous
- Risk for
spontaneous pneumothorax
- Acute silicoproteinosis
- Butterfly edema
pattern
- Air bronchograms
- Hilar/mediastinal
lymphadenopathy
- Progresses
rapidly over months
- Fibrosis, distortion,
bullae, pneumothorax
- Caplan’s
syndrome
- Multiple large
nodules (may cavitate)
- Nodular interstitial
thickening (CWP)
- Bone changes
of rheumatoid arthritis
- Humeral
or clavicular erosions
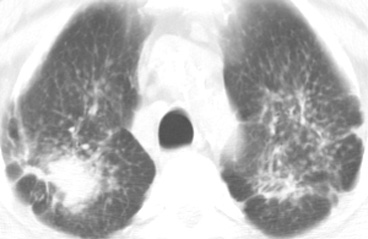
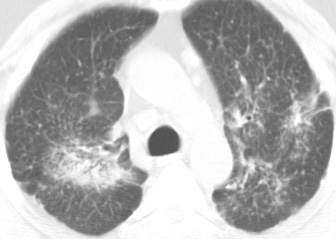
CT/HRCT
- HRCT – best
imaging modality
- Can detect disease
with normal radiograph
- Micronodules
- Upper lobe
and posterior segment predominance
- Location in
center and periphery of lobule
- < 7 mm diameter
- May calcify
- Aggregation of
nodules into PMF more readily detected
- PMF
- Lens shaped
- Nodules >
7 mm
- May cavitate,
- Migrate to
hila with time
- May have punctate
calcification
- Lung distal
to PMF emphysematous
- Hilar/mediastinal
lymphadenopathy, egg shell calcification,
|
| Differential
Diagnosis |
- Sarcoidosis
- TB
- Fungal infection
- Langerhans cell
histiocytosis
- Hypersensitivity
pneumonitis
- Differentiation
- History of occupational
exposure
- Egg shell calcification
only seen with sarcoid
- Langerhans cell
histiocytosis or Farmers lung do not lead to PMF
|
| Pathological
Features |
- General
- Upper lobe
predominance
- Increased risk
of tuberculosis
- Silica more
fibrogenic
- Progressive
massive fibrosis - nodules aggregate, form small and large masses
of fibrosis, sometimes with cavitation
- Silicosis
- Inhalation
of silica dust, silicon dioxide (SiO2)
- Silica particles
within concentric lamellae of collagen in bronchioles, small vessels,
and lymphatics
- Birefringent
silicate crystals (1 – 3 µ) in nodules by polarized
microscopy
- Silica laden
macrophages carry particles to hilar and mediastinal nodes and form
granulomas
- May co-exist
with TB
- Silicoproteinosis
high concentrations of silica, alveolar filling by lipoproteinaceous
material, similar to alveolar proteinosis
- Coal workers pneumonconiosis
- Macule: stellate
shaped collection of macrophages containing black particles, (1
– 5µ) in terminal and respiratory bronchioles and in
pleural lymphatics
- No or little
fibrosis
|
| Clinical
Presentation |
- More common in
men with occupational history of exposure
- Silicosis progressive,
even after removal from dust
- CWP will not prgoress
is removed from dust
- Sandblasting, work
in quarries, mining, glassblowing, pottery making
- Silica often found
in coal mines (silica most common element earth’s crust)
- Acute silicoproteinosis
- Massive exposure
to silica dust
- Usually seen
in sandblasters
- Marked cellular
and exudative alveolar reaction
- Chronic form requires
20 or more years of high dust exposure
- Caplan’s
Syndrome
- CWP, rheumatoid
arthritis, necrobiotic lung nodules
- Symptoms
- None with simple
silicosis.
- Miners commonly
smoke and have symptoms related to bronchitis or emphysema
- Cough, dyspnea,
increased sputum in complicated disease
- Black sputum
in coal workers
- Pulmonary hypertension,
cor pulmonale
- PFTs – decreased
diffusion capacity, obstructive, then restrictive defect
- Diagnosis by history
of exposure, radiography/HRCT and/or lung biopsy
- Slight increased
risk of lung cancer, scleroderma
- Prognosis
- Complicated PMF,
death from respiratory failure, pneumothorax, carcinoma, TB
- Silicosisproteinosis:
death within 2 to 3 years
|
| References |
Pendergrass
EP. Some considerations concerning the roentgen diagnosis of pneujoconiosis
and silicosis AJR 48:571-594, 1942
Remy-Jardin M, Degreef JM, Beuscart R, et al. Coal worker's pneumoconiosis:
CT assessment in exposed workers and correlation with radiographic findings
Radiology 177:363-371, 1990
Bergin CJ, Muller NL, Vedal S, et al. CT in silicosis: correlation with
plain films and pulmonary function tests AJR 146:477-483, 1986
|