| The radiology report is the primary means of communication between the radiologist and the referring physician. The report reflects the attitude, perception and capability of the radiologist and serves as a legal document. Style: Most radiologists use the format: Discussion: Impression This is logical and follows the inductive method. The facts are weighed and a conclusion made. In the modern hospital environment it has disadvantages. Those listening to the report have to wait until the end to hear the conclusion. The same problem is inherent in reading reports online, the referring clinician may have to scroll, or worse, page to the conclusion. A less popular format: Diagnosis or Findings Discussion. This reverse logic brings the most important information to the top where it is seen or heard first. This is the format preferred by the referring clinician. Which ever format is used a few caveats: Be brief. Clinicans have been asked what they want: "brief description of the radiographic findings." Most important finding first. Normal except for cancer RLL is unacceptable. The physician may stop at normal. Quantitate Quantitate Quantitate. Measure if possible or use qualifiers- mild, moderate, severe. Compare, Compare, Compare. Lack of comparison is a common factor in the loss of a malpractice lawsuit. Call Results forunexpected, life-threatening problems call the referring physician. Document the call in the report. Make the referring physician look good - A common phrase "fracture is poorly aligned" should be avoided. Describe the facts. Juries do not understand poorly Don't be vague. Be a journalist and not a reporter. Interpret. Avoid "if clinically indicated." Don't hedge. Put yourself in the referring physician's shoes. What would you conclude if you read this report? |
|||||||||||
| Brevity is the soul of wit Lawyers will argue that reports should be wordy as a defense against malpractice. Short reports equate to haste and carelessness. However, long reports cost money to produce and read. Be succinct. Eliminate unneeded or redundant words. "There is an area of linear atelectasis in the right lower lobe" should be - "Linear atelectasis right lower lobe." Redundancy is common. Example: lung fields. Redundant (and silly concept). "The lung fields are normal" becomes "normal lungs". |
|||||||||||
| Missed cancer conundrum Unfortunately it is not uncommon to find a new malignancy on a mammogram or chest radiograph which in retrospect was present and reported out by a colleague as "normal" Words or phrases to avoid:
|
|
||||||||||
|
|||||||||||
|
The pen is mightier than the sword
|
|||||||||||
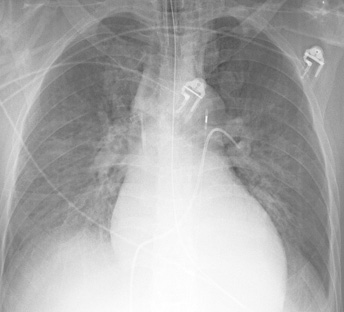
| One of the most effective but least appreciated tools is the grease pencil. Mark up the films. On portables, mark the end of all the lines and catheters. Mark the carina. Mark the edge of the pneumothorax. Outline collapsed lobes and anything else which you feel important. Why? IRed marks help convey what's important. There's a more subtle message that is also relayed. I've been there. I'm involved. I have an interest in patient care. Which brings up the story of kilroy. |
|||||||||||
 |
|||||||||||
| The Legend Kilroy is an American legend. The story began in World War II, where on faraway islands and European battlefields, his name greeted GI's. Wherever GI's kicked up dust or slogged through mud, Kilroy's trademark was there first, and he certainly reached some places even the toughest avoided. The impudent announcement that "Kilroy was here," decorated walls, pillboxes, and any other handy surface from Hitler's "Eagle Nest" at lofty Berchtesgaden to isolated beaches in the far Pacific. Origin |
|||||||||||
| For more information, please refer to the: ACR Standard for Communication: Diagnostic Radiology |
|||||||||||
| References | |||||||||||
|
Smith JP. Risk management for the radiologist. AJR 1987; 149:641-643. Clinger NJ, Hunter TB , Hillman BJ. Radiology reporting: attitudes of referring physicians. Radiology 1988; 169:825-826. Berlin L. Reporting the "missed" radiologic diagnosis: medicolegal and ethical considerations. Radiology 1994; 192:183-187. McLoughlin RF, So CB, Gray RR , Brandt R. Radiology reports: how much descriptive detail is enough? AJR 1995; 165:803-806. Berlin L. Communication of the urgent finding. AJR 1996; 166:513-515. Sobel JL, et al. Information content and clarity of radiologists' reports for chest radiography. Acad Radiol 1996; 3:709-717. Berlin L. Radiology reports. AJRl 1997; 169:943-946. Berlin L. Malpractice issues in radiology. Admitting mistakes. AJR 1999; 172:879-884. Cascade PN , Berlin L. Malpractice issues in radiology. American College of Radiology Standard for Communication. AJR 1999; 173:1439-1442. Berlin L. Comparing new radiographs with those obtained previously. AJR 1999; 172:3-6. Berlin L. Malpractice issues in radiology. Alliterative errors. AJR 2000; 174:925-931. Berlin L. Must new radiographs be compared with all previous radiographs, or only with the most recently obtained radiographs? AJR 2000; 174:611-615. |
|||||||||||
![]()
 Kilroy was here
Kilroy was here